Whiplash can be a disorienting and painful experience, but understanding its recovery timeline can empower you to take an active role in your healing. While individual experiences vary, a structured approach to rehabilitation, guided by expert physiotherapy, is crucial for optimal recovery. From managing acute pain to restoring full function, physiotherapy helps you navigate each week with confidence, transforming injury into an opportunity for greater resilience. At South Island Physio, we are dedicated to helping you achieve thoughtless, careless, and fearless movement after whiplash.
Understanding Whiplash: The Impact on Your Neck and Beyond
Whiplash is a common neck injury that occurs when the head is suddenly and forcefully thrown backward and then forward, often due to a car accident, sports injury, or other trauma. This rapid movement can strain the muscles, ligaments, and joints in the neck, leading to a variety of symptoms [1].
Symptoms of whiplash can include:
Neck pain and stiffness
Headaches often start at the base of the skull
Shoulder pain or tenderness
Dizziness or vertigo
Blurred vision
Fatigue
Difficulty concentrating or memory problems
These symptoms can appear immediately after the injury or develop hours to days later, making early diagnosis and intervention crucial. The unpredictable nature of whiplash can be frustrating, but a clear understanding of the recovery process can provide reassurance and direction.
The Empowering Journey: Whiplash Recovery Week by Week with Physiotherapy
Recovery from whiplash is a dynamic process, and while timelines are approximate, physiotherapy plays a vital role in guiding you through each stage. Our Registered Physiotherapists at South Island Physio specialize in cervical spine rehabilitation, offering personalized care to optimize your healing.
Week 1: The Acute Phase – Managing Pain and Protecting Your Neck
In the initial days following a whiplash injury, pain and stiffness are typically at their peak. The primary goals during this phase are pain management, inflammation reduction, and protection of injured tissues. Your physiotherapist will:
Assess Your Injury: A thorough evaluation to understand the extent of your injury and rule out more serious conditions.
Pain Relief Strategies: Guidance on gentle movements, ice or heat application, and appropriate pain medication (in consultation with your doctor).
Gentle Mobilization: Very light, controlled movements to prevent excessive stiffness and promote circulation without aggravating the injury.
Education: Understanding your injury, what to expect, and how to safely perform daily activities without re-injury.
Weeks 2-6: The Sub-Acute Phase – Restoring Movement and Function
As acute pain begins to subside, the focus shifts to restoring a greater range of motion, strengthening weakened muscles, and improving overall function. This is a critical period for active rehabilitation. Your physiotherapist will introduce:
Progressive Exercises: Gradually increasing neck and shoulder exercises to improve flexibility, strength, and endurance.
Manual Therapy: Hands-on techniques to release muscle tension, improve joint mobility, and reduce stiffness.
Postural Correction: Addressing any compensatory postures that may have developed and providing strategies for optimal alignment.
Return to Activity Guidance: Advice on gradually resuming light daily activities, work, and recreational pursuits, ensuring a safe progression.
Weeks 6+: The Chronic Phase – Building Resilience and Preventing Recurrence
For some, symptoms may persist beyond six weeks, entering the chronic phase. The focus here is on building long-term resilience, addressing any lingering symptoms, and preventing future recurrences. Even if you feel better, continued rehabilitation is key to durable results. Your physiotherapist will:
Advanced Strengthening and Stability: Exercises to build robust neck and core strength, enhancing stability and reducing vulnerability to future injury.
Vestibular Rehabilitation (if needed): Specialized exercises to address any persistent dizziness or balance issues.
Ergonomic Advice: Optimizing your workspace and daily habits to minimize neck strain.
Mind-Body Education: Empowering you with strategies for stress management and self-care, recognizing the interconnectedness of physical and emotional well-being.
South Island Physio: Your Guide to a Resilient Recovery
At South Island Physio, we believe that pain and injury are moments of opportunity; pivot points in your life that help you reach for something greater. Our experienced team of Registered Physiotherapists are dedicated to providing compassionate, evidence-based care, tailored to your best life after whiplash.
We work together with our patients to create personalized treatment plans that can help restore and maintain optimal health. Our goal is to step away from the problems of the past and look to create bright futures of thoughtless, careless, and fearless movement. Let us support your body’s long-term health and help you transform your whiplash recovery into a journey towards a stronger, more resilient you.
Frequently Asked Questions (FAQ)
Should I rest completely after a whiplash injury? While some initial rest may be necessary, prolonged immobilization is generally not recommended. Early, gentle movement under the guidance of a physiotherapist can help prevent stiffness and promote healing. “Relative rest” is often advised, meaning avoiding activities that significantly worsen symptoms.
How can physiotherapy help with whiplash-related headaches? Physiotherapy can address the underlying neck dysfunction that often contributes to whiplash headaches. Techniques include manual therapy to release muscle tension and improve joint mobility, as well as exercises to strengthen neck muscles and improve posture, all of which can reduce headache frequency and intensity.
What if my whiplash symptoms don’t improve? If your symptoms persist or worsen, it’s crucial to communicate this with your physiotherapist and doctor. They can reassess your condition, adjust your treatment plan, and explore other factors that may be contributing to your prolonged symptoms. Persistence and adherence to your rehabilitation program are key.
Can whiplash lead to long-term problems? While most people recover fully from whiplash, a small percentage may experience persistent symptoms, known as chronic whiplash-associated disorder. Early and appropriate physiotherapy intervention significantly reduces the risk of developing chronic issues and promotes a more complete recovery.
Make Your Move Towards a Full Recovery
Don’t let whiplash hold you back. Take control of your recovery and embark on a journey towards renewed strength and fearless movement. Schedule a consultation with our expert Registered Physiotherapists at South Island Physio today. Let us help you understand your needs and create a durable solution that supports your long-term health and well-being.
References
[1] Sterling, M. (2011). A new approach to the management of whiplash-associated disorders. Manual Therapy, 16(1), 5-10. [2] Physiopedia. (n.d.). Whiplash Associated Disorders. Retrieved from https://www.physio-pedia.com/Whiplash_Associated_Disorders
Hip pain is a common companion during pregnancy, but it doesn’t have to define your experience. With safe and effective physiotherapy, you can alleviate discomfort, improve mobility, and navigate your pregnancy journey with greater ease and confidence. Discover how South Island Physio offers personalized, evidence-based solutions to empower expectant mothers, ensuring a comfortable and active pregnancy.
Understanding Hip Pain During Pregnancy: A Natural, Yet Challenging, Phenomenon
Hip pain during pregnancy is a widespread concern, affecting a significant number of expectant mothers. This discomfort can range from a dull ache to sharp, shooting pains in the hips, groin, lower back, or even radiating down the legs. It often intensifies as pregnancy progresses, particularly in the second and third trimesters [1].
Several factors contribute to hip pain during this transformative period:
Hormonal Changes: The body produces relaxin, a hormone that loosens ligaments in the pelvis to prepare for childbirth. While essential for delivery, this increased laxity can lead to instability and pain in the hip and pelvic joints [2].
Weight Gain: The natural increase in body weight places additional stress on the weight-bearing joints, including the hips.
Changes in Posture and Gait: As the uterus expands, your center of gravity shifts, leading to compensatory postural changes and altered walking patterns that can strain the hip muscles and joints.
Muscle Imbalances: Weakness in the gluteal muscles or tightness in hip flexors can exacerbate hip pain.
Sacroiliac (SI) Joint Dysfunction: The SI joints, which connect the sacrum to the pelvis, can become inflamed or misaligned due to ligamentous laxity and altered biomechanics, leading to localized pain.
While common, hip pain can significantly impact daily activities, sleep quality, and overall well-being. Recognizing its causes is the first step towards finding effective relief.
Empowering Relief: Physiotherapy for Pregnancy-Related Hip Pain
Physiotherapy offers a safe, non-invasive, and highly effective approach to managing hip pain during pregnancy. Our Registered Physiotherapists at South Island Physio are skilled in addressing the unique biomechanical changes of pregnancy and provide tailored interventions that prioritize both maternal comfort and fetal safety.
How Physiotherapy Supports a Comfortable Pregnancy:
Personalized Assessment: A thorough evaluation identifies the specific source of your hip pain, whether it’s related to SI joint dysfunction, muscle imbalances, or postural adaptations.
Manual Therapy: Gentle, hands-on techniques can help restore proper joint alignment, reduce muscle tension, and alleviate pain in the hips and pelvis. These techniques are always adapted to be safe and comfortable for pregnant individuals.
Therapeutic Exercise: Targeted exercises strengthen key muscles (e.g., glutes, core stabilizers) and improve flexibility, enhancing pelvic stability and supporting proper posture. These exercises are carefully selected to be safe and beneficial throughout all stages of pregnancy.
Postural Education: Guidance on optimal posture for sitting, standing, and sleeping can significantly reduce strain on the hips and lower back. This includes recommendations for supportive pillows and body positioning.
Activity Modification: Advice on how to safely continue daily activities and exercise, avoiding movements that exacerbate pain while promoting beneficial movement patterns.
Pain Management Strategies: Learning techniques to manage pain at home, empowering you with tools for self-care.
South Island Physio: Your Partner in a Confident Pregnancy Journey
At South Island Physio, we are dedicated to creating a space where expectant mothers are empowered to discover and trust their body’s capacity for change. Our team understands the nuances of pregnancy-related hip pain and is committed to providing compassionate, evidence-based care.
Our physiotherapists will work collaboratively with you to design a personalized treatment plan that focuses on safe, effective strategies to alleviate your hip pain. We aim to not only provide relief but also to build your confidence and resilience, ensuring you can enjoy your pregnancy journey to the fullest. We believe that injury and discomfort, even during pregnancy, can be a pivot point that helps you reach for something greater – a more comfortable, active, and joyful experience.
Frequently Asked Questions (FAQ)
Is physiotherapy safe during pregnancy? Absolutely. Physiotherapy is a safe and highly recommended intervention during pregnancy, provided it is performed by a qualified and experienced therapist who understands prenatal care. Our physiotherapists are trained to adapt treatments to ensure the safety and comfort of both mother and baby.
When should I seek physiotherapy for hip pain during pregnancy? It’s best to seek help as soon as hip pain begins to affect your daily life, sleep, or activity levels. Early intervention can prevent the pain from worsening and improve your overall pregnancy experience.
Can I still exercise with hip pain during pregnancy? In many cases, yes! Your physiotherapist can guide you on safe, appropriate exercises to strengthen supporting muscles and improve flexibility without aggravating your pain. They will help you differentiate between beneficial movement and movements to avoid.
What can I do at home to relieve hip pain? Gentle stretching, applying heat or cold packs, using supportive pillows (especially between your knees when sleeping on your side), and maintaining good posture can offer relief. Your physiotherapist will provide specific home exercises and advice tailored to your condition.
Make Your Move Towards a More Comfortable Pregnancy
Don’t let hip pain overshadow the joy of pregnancy. Take control of your comfort and well-being. Schedule a consultation with our expert Registered Physiotherapists at South Island Physio today. Let us help you understand your needs and create a durable solution that supports you through every stage of your pregnancy, empowering you to embark on a confident and active journey.
References
[1] Wu, W. H., Meijer, O. G., Uegaki, K., Mens, J. M., van Dieën, J. H., Wuisman, P. I., & Ostgaard, H. C. (2004). Pregnancy-related pelvic girdle pain (PPP), I: Terminology, clinical presentation, and prevalence. European Spine Journal, 13(7), 575-589. [2] Marnach, M. L., Ramin, K. D., Ramsey, P. S., & Palmer, R. A. (2003). Characterization of the relationship between joint laxity and hormones in pregnancy. Obstetrics & Gynecology, 101(2), 331-335.
Frozen shoulder (adhesive capsulitis) causes progressive shoulder pain and loss of both active and passive range of motion due to thickening and stiffness of the shoulder joint capsule. It typically follows three stages (freezing, frozen, thawing) and can last 12 to 24 months.
Key points:
Early on, pain and inflammation predominate; later, stiffness becomes the primary concern.
Most people improve over time, but recovery is gradual and requires patience.
Corticosteroid injections can reduce pain and speed early recovery when used in the first few months.
Physiotherapy, including gentle range-of-motion exercises followed by strengthening, is central to treatment.
Surgery is rarely needed.
Emerging research suggests peri-menopausal hormonal changes (especially declining estrogen) may increase the risk of frozen shoulder by affecting inflammation and connective tissue health, helping explain why it’s most common in women aged 45–60.
Bottom line: early diagnosis, stage-appropriate treatment, and consistent rehab lead to meaningful improvement for most people, even though full recovery can take time.
Frozen shoulder, known as adhesive capsulitis, is one of the most frustrating causes of shoulder pain. It presents with shoulder pain and progressive loss of range of motion in both active and passive shoulder movement. Patients with frozen shoulder often report a shoulder that “just won’t move,” particularly when attempting to lift their affected arm, reach across their chest, or place their hand behind their back.
Understanding the timeline and recovery process can significantly reduce fear and improve outcomes.
What Is Frozen Shoulder?
Frozen shoulder, also called adhesive capsulitis, is a condition where the shoulder joint capsule becomes inflamed, thickened, and stiff. The tissue known as the shoulder capsule surrounds the shoulder joint and helps contain synovial fluid, which allows smooth shoulder movement.
In frozen shoulder, the joint capsule and shoulder capsule thicken, lose elasticity, and develop adhesion. This reduces shoulder motion, particularly external rotation, flexion, and abduction. Unlike a rotator cuff tear, which primarily affects active shoulder strength, frozen shoulder limits both active and passive shoulder range of motion.
The hallmark clinical finding in the diagnosis of frozen shoulder is loss of passive shoulder range of motion, particularly external rotation, with a relatively normal shoulder X-ray. It is among the most common shoulder conditions in adults aged 40-65, particularly in women.
The Three Stages of Frozen Shoulder
Frozen shoulder typically progresses through three stages, although timelines vary. 1. Freezing Stage
Duration: typically 4 to 6 months
The freezing stage is marked by increasing shoulder pain, especially at night. The onset of frozen shoulder may seem gradual. Patients often experience shoulder pain with simple daily activities such as dressing or reaching overhead. Inflammation within the shoulder joint capsule causes pain and progressive stiffness.
During this phase, shoulder movement causes pain, and shoulder motion begins to decline. Shoulder flexion, abduction, and external rotation are often the first affected.
2. Frozen Stage
Duration: 4 to 12 months
In this phase, shoulder pain may reduce pain slightly, but stiffness becomes the dominant complaint. The shoulder becomes significantly restricted. Active and passive shoulder motion are both limited.
The capsule continues to thicken, and adhesion formation restricts shoulder mobility. Patients often cannot move their arm behind their back or lift their affected arm overhead. Activities such as reaching across your chest or lying on your back with the arm overhead are difficult.
3. Thawing Stage
Duration: 6 to 24 months
During the thawing stage, shoulder motion gradually improves. Frozen shoulder remains stiff but steadily improves. Most patients experience significant improvement in shoulder mobility and can return to normal activities.
Full return to the normal range of motion may take 12 to 24 months, although some mild residual stiffness may persist.
What Causes Frozen Shoulder?
The exact cause remains under investigation. Frozen shoulder may occur without a clear trigger, known as primary adhesive capsulitis, or develop after trauma, fracture, shoulder dislocation, or when the shoulder has been immobilized. This is called secondary frozen shoulder.
It is also associated with frozen shoulder risk factors such as diabetes, thyroid disorders, and various shoulder pathologies, including rotator cuff tears.
New Research: The Link to Peri Menopausal Hormonal Changes
Recent data suggests a growing link between peri menopausal hormonal changes and frozen shoulder. Estrogen plays an important role in regulating collagen, modulating inflammation, and supporting connective tissue health.
During peri menopause, declining estrogen levels may:
Increase inflammation
Alter collagen metabolism
Reduce synovial fluid production
Affect tissue remodelling
Emerging studies show that adhesive capsulitis is disproportionately common in peri menopausal women. Estrogen receptors have been identified in the shoulder joint capsule, and reduced estrogen may contribute to capsular thickening and fibrosis.
Some preliminary data suggest women receiving hormone replacement therapy may have a lower incidence of frozen shoulder, although more high quality trials are needed. While this does not yet change primary treatment, it provides insight into why this condition peaks between ages 45 and 60.
Diagnosis and Treatment
To diagnose frozen shoulder, clinicians assess active and passive shoulder range of motion. The defining feature is restriction in both active and passive shoulder movement, particularly external rotation.
Imaging is usually normal; however, ultrasound or MRI may reveal thickening of the shoulder joint capsule.
Treatment Options
Frozen shoulder treatment focuses on reducing pain and gradually restoring motion. 1. Pain Management in Early Stage
In the freezing stage, the primary treatment is pain control. A corticosteroid injection applied to the shoulder joint can reduce inflammation and pain. Evidence shows that corticosteroid injection can improve shoulder symptoms and accelerate early recovery when given within the first few months.
Injecting fluid into the shoulder joint, known as hydrodilatation, may also stretch the capsule and improve shoulder mobility.
2. Physiotherapy and Exercise
Physiotherapy is central to assessment and treatment. A structured home exercise program, including range-of-motion and frozen-shoulder exercises, is recommended.
Examples include:
Passive shoulder range of motion using a stick
Shoulder flexion and abduction in supine, lie on your back and assist the arm to lift your affected arm
External rotation stretches
Cross body stretch across your chest
Gentle pendulum exercises
During early phases, aggressive stretching can worsen inflammation. As pain settles, progressive strengthening exercises for the shoulder muscles and rotator cuff are introduced to improve shoulder strength and shoulder and elbow coordination.
3. When Is Surgery Needed?
Surgery for frozen shoulder is uncommon but may be considered if progress plateaus after prolonged conservative care.
Options include:
Manipulation under anesthesia
Arthroscopic capsular release
Both aim to restore shoulder motion by releasing the thickened joint capsule. Most patients do not require surgery.
What Is the Prognosis?
Frozen shoulder can usually improve substantially over time. While traditional teaching suggested it was fully resolved, recent long-term studies indicate that some patients retain mild stiffness. However, most return to normal daily activities.
The key is a well-structured treatment plan tailored to the stage. With appropriate treatment options, gradual progression, and patience, most people experience meaningful recovery.
Final Thoughts
Frozen shoulder, known as adhesive capsulitis, causes significant shoulder pain and stiffness due to thickening of the shoulder joint capsule. It progresses through three stages and may last 12 to 24 months.
New evidence linking peri menopausal hormonal changes to adhesive capsulitis offers insight into why this condition commonly affects midlife women. While research continues, early diagnosis and treatment, including, when appropriate, corticosteroid injection and structured physiotherapy, remain the foundation of care.
If you experience shoulder pain and notice loss of both active and passive shoulder movement, early assessment can help you move your shoulder safely and improve shoulder mobility with less frustration.
Recovering from Frozen Shoulder: Take Action
If you are struggling with shoulder pain and limited movement, you don’t have to wait it out alone. The team at South Island Physiotherapy specializes in assessing and treating frozen shoulder through personalized physiotherapy programs designed to reduce pain, restore motion, and get you back to daily activities safely. Book an appointment today and start your path to a freer, stronger shoulder.
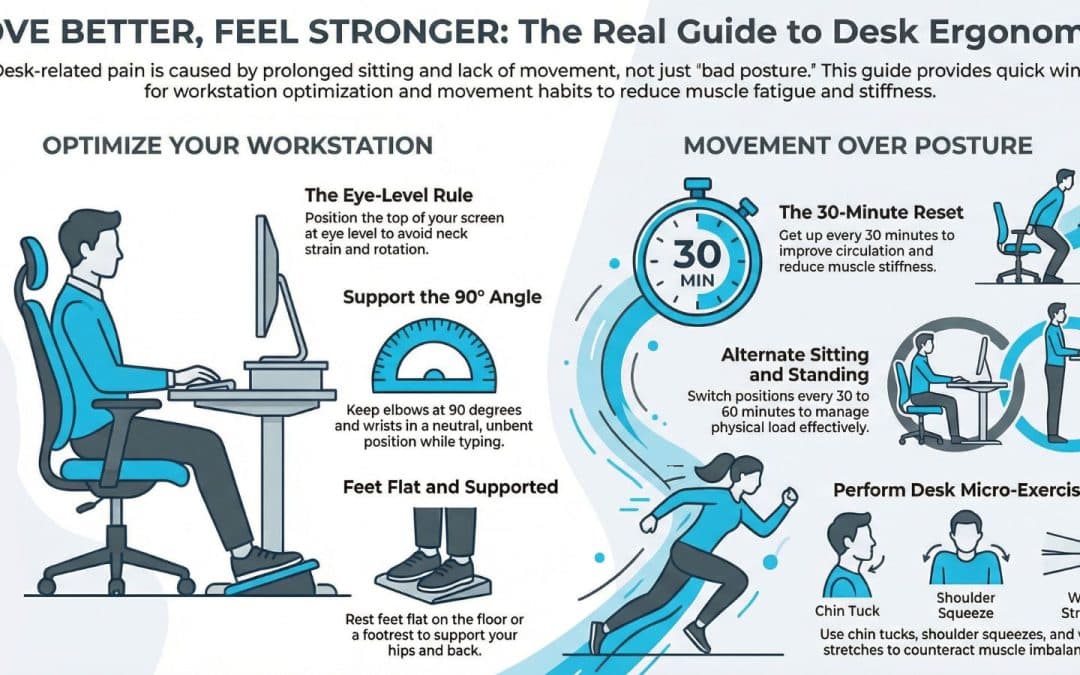
Desk-related neck and back pain is one of the most common reasons people look to improve posture at work. It usually results from prolonged sitting and limited movement, not just “bad posture.” There is no perfect sitting position. The goal is to change positions often, move regularly, and reduce strain through a simple ergonomic desk setup.
Quick wins:
Keep your screen at eye level and elbows around 90°.
Make sure feet rest flat on the floor and chair height supports your hips and lower back.
Alternate sitting and standing if you have a standing desk.
Get up every 30 minutes, even briefly.
Add simple desk exercises for your neck, shoulders, back, and wrists.
Strengthen core and upper back muscles outside of work.
Small, consistent changes beat perfect posture. If pain persists, a physiotherapist can help identify the cause and build a plan to reduce pain and improve how you move at work.
An evidence-based guide to reducing desk-related pain
If you have a desk job, you likely spend hours at a time in a seated position. Prolonged sitting and computer use can contribute to posture issues, neck and back pain, and wrist discomfort. Making small, consistent changes at your workstation can help improve posture and reduce muscle fatigue, tightness, and the risk of chronic pain over time.
The good news is this: posture doesn’t need to be perfect, and small, consistent changes can dramatically reduce pain and discomfort. Below are evidence-based ways to improve your posture and reduce pain from desk work.
1. Understand the Real Cause of Desk-Related Pain
Research consistently shows that pain from desk work is less about a single “bad” sitting position and more about staying in one position for hours. Prolonged sitting reduces blood circulation, increases stiffness, and can overload specific muscle and joint structures in the back and neck muscles.
Common postural patterns seen in desk posture include:
Forward head position, which increases neck strain and pain in your neck
Rounded shoulders or hunched bad posture
Excessive flexion through the lower back
Wrist extension or compression during keyboard and mouse use
These patterns can lead to neck and shoulder pain, lower back discomfort, wrist pain, and even conditions such as carpal tunnel syndrome.
The goal is not perfect posture. The goal is to manage variability and load.
2. Optimize Your Workstation Setup
While there is no perfect workstation, improving your workstation setup can help you maintain a more neutral spine and reduce strain.
Desk and Chair Height
Adjust chair height so your feet rest flat on the floor.
Your knees and hips should be roughly level.
If needed, use a footrest to keep your feet flat and supported.
An ergonomic chair can help support the natural curves of your spine, but it is not a magic fix.
Monitor Position
The top of your screen should be at eye level.
The monitor should be directly in front of you to avoid neck rotation.
If you are using a laptop, elevate it and use an external keyboard and mouse to avoid neck and back strain.
Keyboard and Mouse
Keep your elbow at approximately 90 degrees.
Wrists should remain in a neutral position, not bent upward.
Keep the keyboard and mouse close enough so you are not reaching forward.
These small ergonomic adjustments can significantly reduce desk-related pain and help you sit correctly throughout your workday.
3. Sitting Posture: What Actually Matters
When sitting at a desk, aim for:
A neutral spine, not rigid but upright
Shoulder blades are gently supported rather than aggressively pulled back
Chin slightly tucked rather than jutting forward
Even weight through both hips
However, even a good sitting posture held for hours at a time can lead to muscle fatigue and stiffness. Poor sitting is often simply sitting too long.
Think of correct posture as a moving target. The best posture is your next posture.
4. Use Sitting and Standing Strategically
A standing desk can be helpful, but switching from sitting to standing without breaks does not automatically reduce neck and back pain. Evidence suggests that alternating between sitting and standing is more effective than staying in either position for hours.
Tips to help:
Change position every 30 to 60 minutes
Avoid locking your knees when standing
Keep the monitor at eye level in both positions
Alternating between sitting and standing helps improve blood circulation and reduce tightness in the back and neck muscles.
5. Build in Regular Movement Breaks
The simplest intervention for desk work pain is movement.
Set a reminder to get up every 30 minutes. Walk to refill your water, perform a few desk exercises, or simply stand and stretch.
Regular movement breaks help:
Reduce stiffness
Improve circulation
Decrease muscle fatigue
Prevent neck and back pain from building up
Even 60 seconds of movement can help you feel significantly better.
6. Desk Exercises That Actually Work
Quick desk exercises can help counteract the muscle imbalance created by prolonged sitting.
For Neck and Shoulder Relief
Gently retract your chin to counter forward head posture
Perform shoulder blade squeezes to activate mid back muscles
Slow neck rotations to reduce neck strain
For Lower Back
Stand and extend gently backward
March in place to activate core muscles
Perform seated pelvic tilts to reduce stiffness
For Wrist and Hands
Stretch your hands by extending and flexing the wrist
Shake out your hands
Gently stretch forearm muscles
These exercises support the back and neck muscles and reduce pain and discomfort associated with desk posture.
7. Strength Outside of Work
What you do outside of work matters just as much as your desk setup.
Strength training focused on core muscles, glutes, and upper back can help you maintain better posture during your workday. Regular physical activity also reduces the risk of chronic pain.
Staying active improves muscle endurance, blood circulation, and overall resilience to load. This reduces the likelihood that sitting-related stress will cause pain.
8. When to Seek Professional Help
If you experience persistent back or neck pain, neck pain radiating into the arm, or wrist pain that does not improve with ergonomic changes, consult a physiotherapist.
Physiotherapy can:
Identify the specific cause of your pain
Address muscle and joint dysfunction
Provide individualized desk exercises
Help you improve your posture in a practical way
In some cases, chiropractic care may also provide short-term symptom relief, but long-term improvement typically requires strengthening and movement strategies.
Key Takeaways
Posture right does not mean rigid. It means adaptable.
Pain from desk work is usually the result of prolonged sitting, muscle fatigue, and reduced movement, not simply poor body alignment. A perfect workstation is less important than consistent variability.
To reduce pain:
Optimize your workstation setup
Keep your screen at eye level
Ensure feet rest flat on the floor
Take regular movement breaks
Alternate sitting and standing
Strengthen outside of work
These evidence-based strategies can reduce pain and help you feel more comfortable during your workday.
If desk-related pain is limiting your ability to stay active, a physiotherapist can help you develop a plan tailored to your workspace, work environment, and lifestyle.
You do not need perfect posture. You need sustainable habits to stay mobile, adaptable, and resilient.
Work Smarter. Move Better. Feel Stronger.
If desk-related pain is affecting your focus, sleep, or ability to stay active, the team at South Island Physiotherapy can help. Our physiotherapists take the time to understand your work setup, movement patterns, and daily demands, then develop a personalized plan to reduce pain and improve your body’s tolerance for desk work. From hands-on treatment and targeted exercise programs to practical workstation advice you can actually apply, we can help you move better, feel stronger, and stay productive without chasing “perfect” posture. Book your appointment today!
Sports Massage Techniques That Help Athletes Train Harder and Recover Smarter
Sports massage therapy does not reliably improve strength, speed, or endurance, but strong evidence shows it can reduce muscle soreness (DOMS), improve short-term flexibility, and enhance perceived recovery and relaxation. When delivered by a trained sports massage therapist and integrated with physiotherapy and training, it is a valuable adjunct for recovery, injury prevention, and consistent athletic performance.
For serious athletes, recovery is as important as training load. Sports massage therapy is widely used in sports medicine and physiotherapy settings to support recovery, manage tissue stress, and reduce the risk of injury. While massage is often marketed as performance-enhancing, scientific evidence provides a more nuanced and practical picture.
What the Evidence Actually Shows
A large systematic review and meta-analysis of 29 randomized controlled trials (enrolling over 1,000 participants) found that sports massage does not meaningfully improve objective performance measures, such as strength, sprint speed, endurance, or fatigue. However, it produces small but significant reductions in delayed-onset muscle soreness (DOMS) and improvements in flexibility compared with no intervention (Davis et al., 2020).
A more recent systematic review focusing on massage therapy in sport confirmed these findings, noting consistent benefits in pain reduction, relaxation, and perceived recovery, even when physiological markers such as lactate clearance and muscle activation showed mixed or minimal effects (Guo et al., 2023).
In short, sports massage helps athletes feel and move better, even if it does not directly make them faster or stronger.
How Sports Massage Supports Athletic Recovery
Reduced Muscle Soreness (DOMS) DOMS can limit training frequency and quality. Evidence consistently shows that massage reduces perceived soreness following intense physical activity, supporting faster return to training.
Short-Term Flexibility Gains Massage can temporarily improve joint range of motion and soft-tissue extensibility, which is useful before training blocks or competition, especially in sports requiring repetitive movement or large ranges of motion.
Nervous System and Relaxation Effects Massage appears to influence the autonomic nervous system, promoting relaxation and reduced stress. This neural effect may support recovery by improving sleep quality and readiness between sessions.
Load Management and Injury Prevention While massage does not treat injuries directly, it can help manage tissue tone, muscle balance, and tightness, potentially lowering the chance of overuse strain when combined with proper training and physiotherapy.
Deep Tissue, Athletic Massage, and Clinical Integration
Deep tissue massage, trigger point therapy, active release, cupping, and mobilization are commonly used in sports massage therapy. Evidence suggests that regular, targeted massage, rather than one-off sessions, may provide greater benefits for flexibility and soreness, particularly in high-volume or elite athletes.
Sports massage works best as an adjunct, not a replacement, for physiotherapy, rehabilitation, strength training, and load management. In a multidisciplinary clinic, massage therapists and physiotherapists can coordinate care to align treatment with anatomy, biomechanics, and individual athletic demands.
FAQ: Sports Massage Therapy
Does sports massage improve athletic performance? Not directly. Research shows little consistent improvement in strength, speed, or endurance. Its value lies in recovery, reduced soreness, and increased flexibility.
Is sports massage better than regular relaxation massage? Yes, for athletes. Sports massage is tailored to specific muscle groups, movement mechanics, and training loads, unlike general Swedish or relaxation massage.
How often should athletes get sports massage? Evidence suggests regular massage, such as weekly or bi-weekly during heavy training, is more effective than occasional sessions, especially for chronic tightness or repetitive strain.
Is sports massage useful for injury rehab? As an adjunct. It can help manage pain, muscle tension, and tissue sensitivity, but it should be combined with physiotherapy and progressive loading for effective rehabilitation.
How long should a sports massage session be? Most effective sessions range from 60 to 90 minutes, allowing adequate assessment, targeted treatment, and recovery-focused work.
Who should provide sports massage? A certified, registered sports massage therapist who understands anatomy, sports therapy principles, and collaborates with physiotherapy or sports medicine professionals.
Recover Smarter With Sports Massage at South Island Physiotherapy
At South Island Physiotherapy, sports massage is integrated into evidence-based physiotherapy care to support recovery, manage training load, and help athletes stay consistent in their sport. Our registered massage therapists and physiotherapists work collaboratively to ensure sports massage therapy complements your training, injury prevention, or rehabilitation plan. Whether you are managing muscle soreness, preparing for competition, or recovering between intense sessions, sports massage at South Island Physiotherapy in Victoria, BC is designed to help you move better, feel better, and train with confidence. Book an appointment today and make recovery part of your performance strategy.
Understanding Risk, Prevention, and Evidence-Based Management of Growth Spurts
Growth spurts are a defining feature of childhood and adolescence. For young athletes, periods of rapid growth can bring exciting improvements in height and athletic performance, but they also carry a temporary increase in injury risk. Growth-related injuries occur when the musculoskeletal system struggles to adapt to rapid bone growth, changing biomechanics, and increasing training demands.
This article explains how growth spurts can cause a range of injuries, why injuries tend to cluster during adolescence, and how parents, coaches, and clinicians can reduce the risk through evidence-based injury prevention and treatment strategies.
Adolescent Growth Spurt and Peak Height Velocity
During adolescence, children experience periods of rapid growth in stature known as growth spurts. The most critical window is peak height velocity, the point at which growth in stature and bone growth occur at their fastest rate. For most children, this occurs earlier in girls than in boys, but the timing varies widely.
Rapid bone growth can temporarily outpace the ability of muscles and tendons to lengthen and adapt. This mismatch between bone growth and soft tissue adaptation is a key contributor to growth-related injuries. Growing bones, especially at the growth plate and apophyses, are more vulnerable to overload and traction injuries during this stage of physical development.
Why Growth Spurts Increase Injury Risk
Research in youth sport consistently shows that injury rates rise during periods of rapid growth. Several factors contribute to this increase in injury risk.
Growth plate vulnerability
The growth plate is a region of developing cartilage near the ends of long bones. Growth plate injuries are more likely than ligament injuries in children and teenagers because these areas are structurally weaker than the surrounding bone. Fracture risk, including stress fractures, increases when repetitive loading exceeds the tissue’s capacity.
Mismatch between bone growth and soft tissue
Rapid bone growth can lead to relative tightness in muscles and tendons. Factors include poor flexibility of the quadriceps, hamstrings, and calf muscles. This imbalance increases strain on tendons, ligaments, and apophyseal regions.
Overuse and overload
Overuse injuries and burnout are common in youth sport, especially when training volume increases without adequate recovery. Overuse injuries that often occur during adolescence often involve repetitive running and jumping, such as in soccer, basketball, volleyball, and track.
Changes in coordination and velocity
During periods of rapid growth, coordination can temporarily decline. Changes in limb length, center of mass, and movement velocity can increase non-contact injuries and acute injuries during sports and physical activities.
Common Growth-Related Injuries in Young Athletes
Growth-related injuries include both acute and overuse injuries. Injuries observed during adolescence often involve the growth plate, tendon, or bone-tendon junction.
Osgood-Schlatter disease: Osgood-Schlatter disease is a traction injury at the tibial tuberosity and is one of the most well-known growth-related conditions. It is a serious overuse injury seen in running and jumping sports. Pain occurs where the patellar tendon attaches to the growth plate of the shin bone.
Sever’s disease: Sever’s disease involves the calcaneal growth plate in the heel. It is common among children and teens who participate in high-volume running sports. It is classified as an apophyseal injury and is linked to rapid bone growth, tight calf muscles, and high training loads.
Apophyseal injuries: Apophyseal injuries occur where muscles and tendons attach to bone. These traction injuries are common during periods of rapid growth when muscular strength increases faster than tendon adaptation.
Stress fractures: Stress fractures are overuse injuries caused by repetitive overload. Injury rates increase during adolescence when rapid bone growth temporarily reduces bone strength relative to loading demands.
Muscle strains and soft tissue injuries: Muscular strain and ligament injuries can occur when strength, flexibility, and neuromuscular control lag behind physical changes. Injuries in young athletes often involve the lower limb during growth spurts.
Evidence on Injury Rates in Youth Athletes
High-quality studies in sports medicine show that injuries in youth athletes are not evenly distributed across age groups. Injury rates are higher around peak height velocity compared to pre-pubertal or post-maturation stages. Injuries compared across age groups consistently show a higher risk of developing both acute and overuse injuries during adolescent growth spurts.
Research also suggests that injuries occur more frequently in athletes who specialize early, train year-round, or experience rapid increases in training volume without adequate recovery.
Injury Prevention During Growth Spurts
Prevent injuries by focusing on load management, physical preparation, and education.
Monitor growth and maturity: Tracking stature growth helps identify periods of rapid growth. Awareness of peak height velocity allows coaches and clinicians to proactively adjust training loads.
Manage training load and overload: Reduce the risk by avoiding sudden spikes in volume or intensity. Overuse injuries and burnout are strongly linked to excessive load without recovery.
Strength and conditioning: Evidence supports the use of appropriately supervised resistance training for children and adolescents. Strength training improves tendon and ligament capacity, enhances neuromuscular control, and reduces injury risk when performed correctly.
Address flexibility and imbalance: Factors include poor flexibility of the quadriceps, calves, and hamstrings. Targeted mobility work can reduce strain on growth plates and soft tissue structures.
Emphasize movement quality: Strength and conditioning programs should focus on technique, coordination, and control rather than maximal loading during periods of rapid growth.
Injury prevention and treatment strategies: Early recognition is key. Pain that persists, worsens with activity, or affects athletic performance should not be ignored. Injury prevention and treatment should prioritize relative rest, gradual return to sport, and addressing contributing factors such as overload, imbalance, and poor movement patterns.
Soft tissue massage may help relieve symptoms, but it should be used as part of a broader management plan that includes load modification and strength training.
Key takeaways for Parents, Coaches, and Young Athletes
Growth-related injuries occur most commonly during adolescent growth spurts and peak height velocity
Rapid bone growth can increase injury risk due to a mismatch between bone growth and muscles and tendons
Overuse injuries, apophyseal injuries, stress fractures, and growth plate injuries are common during adolescence
Injury prevention strategies that focus on load management, strength and conditioning, and flexibility can reduce injury risk
Understanding and managing growth and development is essential for long-term athlete development and athletic performance
Injury Prevention and Care During Growth Spurts
If your child or teen is experiencing pain, recurring injuries, or performance changes during a growth spurt, early assessment and guided management can make a significant difference. At South Island Physiotherapy, our team provides evidence-based physiotherapy, injury prevention programs, sport-specific rehabilitation, and strength and conditioning support tailored to growing athletes. We work closely with young athletes and families to manage load, restore movement quality, and support a safe return to sport during periods of rapid growth. Book an appointment today to ensure your athlete stays healthy, confident, and active through every stage of development.